
In this month’s installment of our Therapeutic Cheat Sheet Series, we turn our focus to rosacea. Antibiotics have been a mainstay for rosacea treatment for decades, but their side effect profile and dosing schedules can complicate their use. Enter Doxycycline-Modified Release (Doxy-MR). This specialized formulation of doxycycline allows for sustained activity and a minimized side effect profile in one daily dose.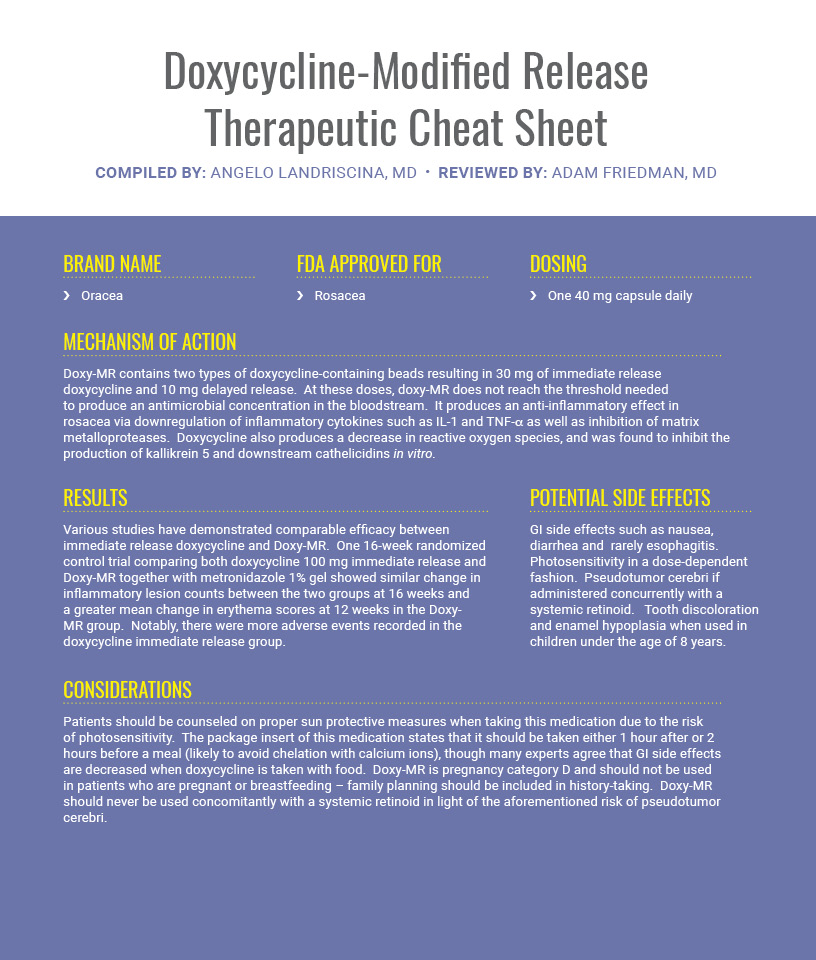
If you would like to read more about Doxycycline , check out the following articles published in the Journal of Drugs in Dermatology:
![]()
The Use of Oral Antibiotics in the Management of Rosacea
Rosacea is common inflammatory facial dermatosis. Rosacea has variable manifestations including facial flushing, central facial erythema, telangiectasias, and papulopustular lesions. Treatment of rosacea is challenging given the varied manifestations and incompletely understood etiology, but the treatment of papulopustular presentations often relies on oral antibiotics. Tetracyclines, specifically doxycycline, are the most commonly prescribed antibiotics for rosacea. Other antibiotics that can be used include macrolides, commonly azithromycin, and rarely, metronidazole. This paper will review the evidence for the use of antibiotics in the treatment of rosacea.
INTRODUCTION: Routine use of doxycycline (DC) 100 mg for the treatment of moderate to severe acne may be associated with gastrointestinal adverse events (AEs), thus potentially impacting patient adherence, and antibiotic resistance. This study evaluated the safety and efficacy of subantimicrobial, modified-release (MR) DC 40 mg compared to DC 100 mg and to placebo for the treatment of inflammatory lesions in moderate and severe acne.
METHODS: 662 subjects aged 12 years or older with moderate to severe acne received subantimicrobial, MR-DC 40 mg tablets, DC 100 mg capsules, or placebo once daily for 16 weeks.
RESULTS: MR-DC 40 mg was superior to placebo in the mean reduction of the number of inflammatory lesions, median percent reduction in inflammatory and total lesions, and success rate. MR-DC 40 mg was also comparable to DC 100 mg in the reduction of the number of inflammatory lesions, and percent reduction of total lesions. Incidence of drug-related AEs for MR-DC 40 mg was similar to placebo and was markedly smaller compared to DC 100 mg.
DISCUSSION: MR-DC 40 mg demonstrated comparable efficacy and superior safety to DC 100 mg in the treatment of moderate to severe inflammatory acne.
Rosacea is often under-recognized or misdiagnosed in patients with skin of color (Fitzpatrick Skin Types [FST] IV-VI). Subtle clinical features and a low index of suspicion likely contribute to less frequent diagnosis in this population. Clinical trials of therapeutic agents for rosacea generally include few patients from nonwhite racial/ethnic groups and therefore, potential differences in treatment outcomes have not been previously studied. The objective of this prospective analysis was to fill the gap in knowledge of the effectiveness and safety of treatment for rosacea in patients with skin of color. We analyzed data from 826 adults aged ≥18 years with papulopustular (subtype 2) rosacea (663 FST I-III; 163 FST IV-VI). All patients received doxycycline 40 mg capsules (30 mg immediate release and 10 mg delayed release beads) once daily as monotherapy for 12 weeks in this open-label, multicenter, community-based study. Investigators assessed disease severity with the Investigator’s Global Assessment (IGA) and erythema with the Clinician’s Erythema Assessment (CEA). Significant improvement in disease severity and erythema was obtained in patients with FST I-III and IV-VI at week 12 (P<.001). Treatment success, defined as an IGA score of 0 or 1 was achieved in 74.6% and 74.3% of patients with FST I-III and IV-VI, respectively. Approximately 12% of patients experienced adverse events with no difference between the two skin type groups. The results of this prospective subgroup analysis of data from a large community-based trial suggest that doxycycline produced similar effectiveness and safety profiles in patients with FST I-III and IV-VI.
Did you enjoy cheat sheet? You can find more here.