Learn more about what it’s like to be a dermatologist today and what it takes to transition from residency to being a practicing dermatologist.
Find hands-on clinical pearls to help you care for your patients more effectively, stay up-to-date with the latest research, or stop by often for expert advice from industry leaders and insights on what it takes to be a key opinion leader.
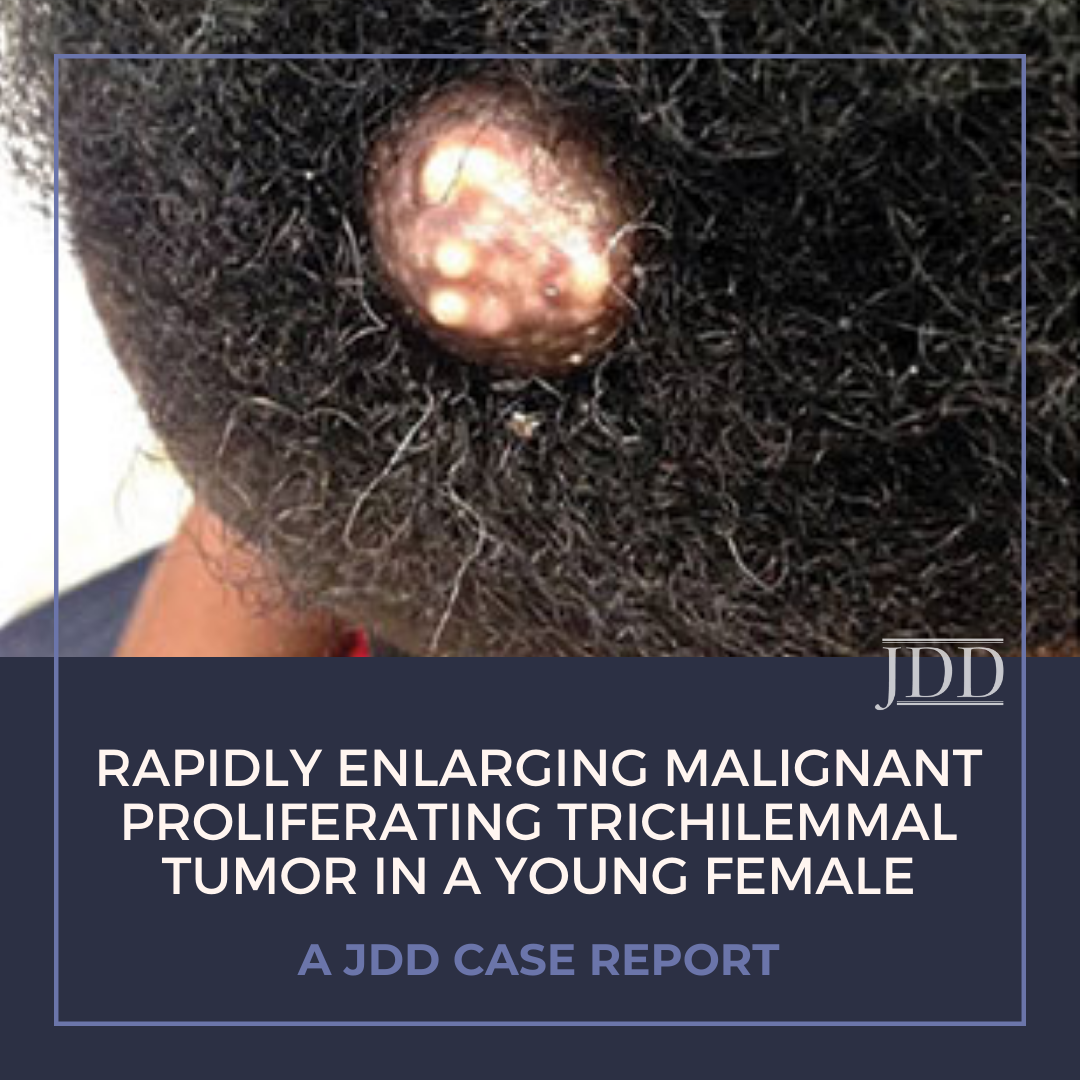
Malignant proliferating trichilemmal tumors are rare adnexal neoplasms that most commonly occur on the scalp in elderly women. These tumors are associated with recurrence and even nodal or distant metastatic spread. Here, JDD authors describe a 38-year-old patient who presented with a scalp nodule that was diagnosed as a high-grade malignant proliferating trichilemmal tumor.
Introduction
This observation describes the presentation, histopathologic diagnosis, and treatment of a malignant proliferating trichilemmal tumor.
Clinical Presentation
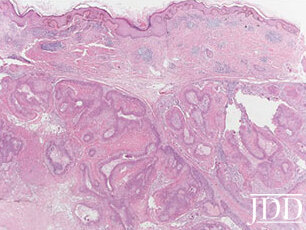
A 38-year old female presented with a several-year history of an enlarging, firm, and occasionally painful lesion on her left scalp (Figure A). The patient denied any bleeding or drainage from the nodule. There was no personal or family history of skin cancer. On physical exam, a 3 cm x 3 cm x 1.5 cm, well-demarcated, brown-colored multinodular, dermal lesion was noted on the patient’s left scalp. It was not ulcerated or fixed to underlying bone. A shave biopsy was performed, and histopathologic examination of the specimen revealed abrupt trichilemmal keratinization without a granular cell layer, cysts with homogenous keratin, and multiple, broad, anastomosing bands of nodules and lobules. Furthermore, pleomorphism with nuclear atypia, increased abnormal mitotic figures, hyper- chromatism, and necrotic cells led to the diagnosis of malignant proliferating trichilemmal cyst (Figure B). The patient elected for complete surgical excision given the histopathologic diagnosis. The patient continues to be closely monitored for recurrence and/or metastasis.
FIGURE A. Brown nodule with irregular lobulated granular surface with cream-colored fields on top.
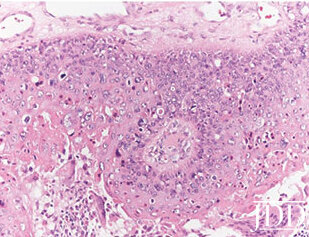
FIGURE B. Multinodular dermal neoplasm with trichilemmal squamous differentiation and no connection to the epidermis (original magnification x20).FIGURE C. Neoplastic keratinocytes with pale cytoplasm, mild cytologic atypia, and necrotic cells (original magnification x200).
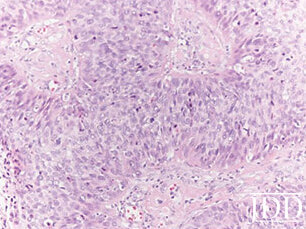
FIGURE D. Poorly differentiated deeper component of tumor with atypical mitoses (original magnification x200).
Discussion
Wilson-Jones first described these tumors in 1966 as proliferating epidermoid cysts.1 Pilar cysts originate from the isthmus of the outer follicular hair root sheath, giving rise to the term trichilemmal cyst or tumor.2,3 Several years later, Saida et al introduced the classification of the malignant proliferating trichilemmal cyst to describe a trichilemmal tumor that was infiltrative and metastatic with histopathologic features of atypia and increased mitotic activity.4,5 While benign pilar cysts are fairly common, affecting roughly 5-10% of the population, transformation into the malignant counterpart or de novo malignancies are extremely rare. Classically, these tumors are found on the scalp in females during their 8th to 9th decade of life.3,6
Ye et al examined 76 proliferating trichilemmal tumors (PTT) in order to outline histopathologic features that could predict clinical behavior and prognosis.7 Three distinct PTT variants were described based on malignant features such as nuclear atypical, mitotic activity, and presence of necrosis. Group I lesions are considered benign with recurrence not observed. Histopathologic examination reveals trichilemmal keratinization, focal nuclear atypia, mononuclear infiltrates, and absence of mitotic figures, perineural invasion, or vascular invasion. Group II lesions are low-grade malignant tumors with an increased risk of local recurrence. Histologically, these tumors are noted to have abrupt keratinization, areas of single-cell necrosis, and desmoplastic stroma. Cytologic atypia is absent. Group III lesions are high-grade malignant tumors with a high risk of recurrence, lymph node involvement, and/ or distant metastasis. Group III tumors infiltrate into the dermis and have abrupt keratinization with regions of multifocal necrosis. Atypical mitoses and a desmoplastic stroma are also present. Because histological examination of our patient’s lesion demonstrated abnormal mitotic figures, cytologic atypia, and necrosis it was considered a Group 3 (high-grade) tumor based on the criteria proposed by Ye et al.
Distinguishing the variant of PTT using histologic examination is important, as no specific clinical criteria currently exist to differentiate benign and malignant tumors. Clinical signs that suggest a poor prognosis include rapidly enlarging tumors, tumors greater than 5 cm in diameter, location other than the scalp, and areas of necrosis on physical examination.8Histological features that favor malignant proliferating trichilemmal tumor (MPPT) include trichilemmal keratinization, lobular growth, and clear demarcation from surrounding structures.8,10 Studies have suggested that immunohistochemical markers such as CD34, Ki-67, and P53 can be used to diagnose MPTT versus squamous cell carcinoma (SCC) and to determine the malignant potential of the lesion.3,8,11 Distinguishing MPTTs from SCC is particularly important as the risk of recurrence and the risk of metastasis are very different between the two. In two case series, the reported rate of metastasis for Group III MPTTs, like that seen in our patient, was approximately 25%.4 Alternatively, in cutaneous squamous cell carcinoma the risk of metastasis is much lower at approximately 1.9-2.6%.12 More research is required before these immunohistochemical markers are used in clinical practice. Wide surgical excision with 1 cm margins is the treatment of choice. Patients should be followed closely to monitor for recurrence and/or metastasis. Case reports utilizing adjuvant chemotherapy/radiation have been published in patients that presented with metastasis and aggressive malignant tumors.13,14 These adjuvant therapies should be used on a case-by-case basis as no clear clinical or pathological guidelines have identified when these treatments are indicated. Mohs micrographic surgery has also been reported as a successful treatment modality in at least one case of a MPTT with local imagining recommended to investigate for regional metastases.15
The clinical course and prognosis of trichilemmal tumors are determined by the histopathological variant as discussed previously and the presence of metastasis at presentation. Surgical excision of benign, Group I trichilemmal tumors is curative.2 Group II and III proliferating trichilemmal tumors require more aggressive monitoring following surgical excision.4 Two studies have discussed the role of Ki-67 immunostaining in determining a tumor’s risk of recurrence and extension.3,11 These studies have found that Ki-67 positive tumors have a worse prognosis and Ki-67 immunostaining may be useful for guiding treatment and monitoring of more high-risk tumors.
Although malignant proliferating trichilemmal tumors most commonly occur in the 8th to 9th decade of life, we present a case of a high-grade tumor occurring in a 38-year-old woman. Given the risk of recurrence and metastasis in such lesions, appropriate identification of this rare neoplasm in younger patients will hasten treatment and improve prognosis.
References
Jones EW. Proliferating epidermoid cysts. Arch Dermatol. 1966;94(1):11-9.
Ramaswamy AS, Manjunatha HK, Sunilkumar B, and Arunkumar SP. Morphological spectrum of pilar cysts. N Am J Med Sci. 2013;5(2):124-8.
Rangel-Gamboa L, Reyes-Castro M, Dominguez-Cherit J, and Vega-Memije E. Proliferating trichilemmal cyst: the value of ki67 immunostaining. Int J Trichology. 2013;5(3):115-7.
Saida T, Oohara K, Hori Y, and Tsuchiya S. Development of a malignant proliferating trichilemmal cyst in a patient with multiple trichilemmal cysts. Dermatologica. 1983;166(4):203-8.
Goyal S, Jain BB, Jana S, and Bhattacharya SK. Malignant proliferating trichilemmal tumor. Indian J Dermatol Venereol. 2012;57(1):50-2.
Sharma R, Verma P, Yadav P, and Sharma S. Proliferating trichilemmal tumor of scalp: benign or malignant, a dilemma. J Cutan Aesthet Surg. 2012;5(3):213-5.
Ye J, Nappi O, Swanson PE, Patterson JW, and Wick MR. Proliferating pilar tumors: a clinicopathologic study of 76 cases with a proposal for definition of benign and malignant variants. Am J Clin Pathol. 2004;122(4):566-74.
Deshmukh BD, Kulkarni MP, Momin YA, and Sulhyan KR. Malignant prolifer- ating trichilemmal tumor: a case report and review of literature. J Cancer Res Ther. 2014;10(3):767-9.
Rao S, Ramakrishnan R, Kamakshi D, Chakravarthi S, Sundaram S, and Prathiba D. Malignant proliferating trichilemmal tumour presenting early in life: an uncommon feature. J Cutan Aesthet Surg. 2011;4(1):51-5.
Chikhalkar S, Garg G, Gutte R, and Khopkar U. Sebaceous carcinoma of scalp with proliferating trichilemmal cyst. Indian Dermatol Online J. 2012;3(2):138-40.
Park BS, Yang SG, and Cho KH. Malignant proliferating trichilemmal tumor showing distant metastases. Am J Dermatopathol. 1997;19(5):536-9.
Brougham NDLS, Dennett ER, Cameron R, Tan ST. The incidence of metas- tasis from cutaneous squamous cell carcinoma and the impact of its risk factors. J Surg Oncol. 2012;106(7):811-815.
Durairaj AR, Mahipathy SR, Vivakaran TT, Harikrishnan V, and Esakki M. Ma- lignant proliferative trichilemmal tumour of the nape of the neck – a case report. J Clin Diagn Res: JCDR. 2016;10(2):PD19-20.
Dubhashi SP, Jadhav SK, Parasnis A, and Patil CS. Recurrent malignant prolif- erating trichilemmal tumor with lymph node metastasis in a young woman. Postgrad Med J. 2014;60(4):400-2.
Fieleke DR, Goldstein GD. Malignant proliferating trichilemmal tumor treated with Mohs surgery: proposed protocol for diagnostic work-up and treat- ment. Dermatol Surg. 2015;41(2):292-294.